 Request an Appointment
Request an Appointment
 215-343-3223
215-343-3223
Terminology
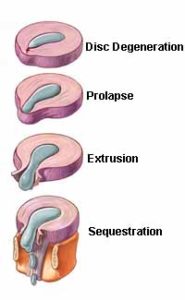
Some of the terms commonly used to describe the condition include:
- herniated disc.
- prolapsed disc.
- ruptured disc.
- “slipped disc.”
Other terms that are closely related include
- disc protrusion.
- bulging disc.
- pinched nerve.
- sciatica.
- disc disease.
- disc degeneration.
- degenerative disc disease.
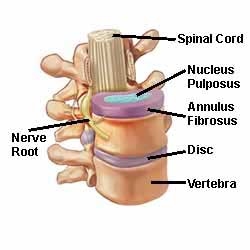
The popular term “slipped disc” is quite misleading. An intervertebral disc is tightly sandwiched between two vertebrae. So it cannot actually “slip,” “slide,” or even get “out of place.” The disc is actually grown together with the adjacent vertebrae. Therefore it can be squeezed, stretched, and twisted, all in small degrees. It can also be torn, ripped, herniated, and degenerated. But it cannot “slip.”
CERVICAL DISC HERNIATION
Cervical disc herniations occur in the neck, most often between the sixth and seventh cervical vertebral bodies. Symptoms can affect the back of the skull, the neck, shoulder girdle, and the scapula. Symptoms can also produce shoulder pain, arm pain, and hand pain.
THESE TESTS MAY INCLUDE THE FOLLOWING :
- X-ray
- Computed tomography scan (CT or CAT scan)
- Magnetic resonance imaging (MRI)
- Myelogram
- Electromyogram and Nerve conduction studies (EMG/NCS)
